Against Maximum Stimulation- Egg freezing, IVF, and the case for gentler fertility medicine.

Why you should read this
This essay is long. As far as I can find, there is little patient-facing writing that puts egg freezing, embryo banking and stimulation protocols all in one place. Most of what exists is heavy on narrative and light on data. I tried to write the opposite.
If you are considering an elective fertility procedure — one that will cost you (or your insurer) thousands of dollars and ask you to take on a course of hormone doses far higher than the body would ever produce on its own- the procedure deserves more than the one-hour consultation you will get with the clinic that profits from doing it.
This essay is also for the women who have already decided that egg freezing or IVF isn’t for them. Many women rule out the procedure because the only version they have ever been shown is the maximally aggressive American one: twenty to forty (or more) injections, estradiol levels five to ten times physiological baselines, weeks of feeling chemically not-yourself. That version is real, and ruling it out is a defensible reaction. But it isn’t the only version.
A woman freezing eggs in much of Europe or Japan is likely to receive substantially less hormonal stimulation per cycle — often half or less — than a woman undergoing the same procedure in the United States, without good evidence that the American approach produces better outcomes per egg or per live birth.I went into this research expecting to confirm my own decision never to do egg freezing, and ended up doing embryo banking on a gentle protocol that I didn’t know existed when I started.
It's worth noting that this essay would not exist without AI as a research tool and writing partner. What took months would have taken years, or more likely, never happened.But the first answer an AI gives on a research question is almost always, and often dangerously so, the most-repeated version of a claim, not the best-evidenced one. To escape this, I had to go to the studies themselves and use AI to interrogate them directly on actual data, sample size, funding, and general study robustness. Used this way, as a conversational tool against sources, AI became a research multiplier rather than an authority.The longer methodology note is in the appendix. I flag it here because the same hands and frontier tools that helped produce this essay could just as easily have produced the opposite one: a well-cited, internally coherent defence of the standard American IVF protocol, if I had not interrogated every confident AI answer.
Reading this end-to-end is a 1–2-hour commitment. Not all of it is relevant to everyone, so every chapter has a title and section headers. Most chapters take 8 to 15 minutes each.Nearly every woman thinks about her fertility at some point, even if she doesn’t mention it. Consider sharing this research with other women in your life, so they can digest it and make more informed decisions.
I had no idea how many people were thinking about egg freezing or IVF, even friends immediately around me, until I started sharing that I was researching it.
How to read this
Skip to whichever chapters are useful to you.
- A primer on how ovaries actually work. Most women going through fertility treatment carry a much shallower understanding than they realize, and that shallowness is what makes the rest of the system so easy to mis-sell.
- Chapter 1: AMH does not measure your fertility. It is a stimulation-response test being sold as a fertility test.
- Chapter 2: Before you start any cycle, fix what’s upstream. Sleep, stress, energy availability, untreated thyroid issues, and a long list of cheap labs that almost no US fertility clinic will run before they put you on a stimulation protocol.
- Chapter 3: The egg-freezing insurance premium is more expensive than it looks. The premium is paid in dollars, in hormone exposure, and in long-term safety uncertainty.
- Chapter 4: You probably do not need all those shots. Fertility clinics in other countries get comparable outcomes with a fraction of the hormonal exposure that American clinics use by default.
- Chapter 5: More eggs ≠ better. Why the “freeze twenty eggs” benchmark is not as settled as it sounds.
- Chapter 6: What we still do not know about long-term hormone exposure. If extra doses do not clearly improve outcomes, the safety question becomes sharper: why take more exposure than necessary?
- Chapter 7: IVF is not automatically safer than conception. ICSI, fresh vs frozen, and the belief that more technological mediation equals lower risk.
- Chapter 8: Why the American system pushes intensity. SART metrics, employer benefits, VC-funded clinics, and injection-count culture.
- Chapter 9: What this leaves for an American patient. What I did, whether travelling makes sense, and the questions worth asking before a cycle.
- Chapter 10: Why the current model may look outdated within a decade. The future of women’s health lies in extending the working life of the ovary. Everything else, eventually, becomes unnecessary.
- Appendix: A note on methodology, and the limits of AI.
Why I wrote this
As a woman in my thirties, I have watched dozens of friends go through egg freezing, embryo banking, and IVF. Most had neutral experiences. Except there was a friend who nearly died from ovarian hyperstimulation syndrome, a complication of the high-dose hormonal stimulation. Another close friend told me the medications made her feel suicidal for the only time in her life.
Intuitively, and I’m often wrong on these things, it felt risky that women took huge doses of hormones, so I decided I’d never do it. Then, earlier this year, at a routine fertility check, a clinic told me my AMH had dropped, and I needed to begin an aggressive IVF protocol immediately. At the time, I barely understood what AMH measured. Like most women, I knew it only as a fertility marker I’d been encouraged to track. Once I started reading the literature around it, the fertility industry began to unravel.
I want to be healthy and have healthy children. My stake in getting the answers right is enormous. Academic researchers and the pharmaceutical companies that fund them often operate under conflicting incentives: expanding markets, defending priors, securing the next grant. The people writing the papers and running the trials almost never have to swallow the pills, take the injections, or live inside the bodies their conclusions shape.Recently, Works in Progress released “We’re freezing our eggs; maybe you should too.” which went somewhat viral- the X thread alone passed a million views. I respect the publication and the authors, but by the time I read it, I’d already come to believe that the recommendation it made (get 20 eggs!), without questioning the doses and protocols standard in the United States, it was not the one most women should receive. Seeing it land that hard pushed me to finish writing this piece.
The goal of this essay is not to argue that fertility preservation is inherently wrong, but that American women are being pushed toward the most aggressive version and the risks that come with that, without being shown meaningful choices.
It's worth saying that most people in the fertility industry are sincere — doing their best inside a system that pays them for volume, rewards them for fallible metrics, and trains them on protocols that have drifted upward over thirty years. It's staffed by good people working inside a structure that produces the wrong defaults
Primer: How ovaries actually work
Most people, myself included at the start of this research, have a much shallower understanding of this than they realise, and that shallowness is what makes the rest of the system so easy to mis-sell.
A female fetus reaches her peak egg count before she is even born, in the second trimester. From that point on, the number declines through the rest of fetal development until menopause. The losses are continuous. They happen every day, regardless of whether a woman is on birth control, pregnant, breastfeeding, ovulating, or doing nothing reproductive at all. The system is built around massive overproduction and massive loss. Throughout an entire reproductive life, only a few hundred eggs will ever ovulate; the body reabsorbs the rest through programmed cell death, which runs quietly in the background.
Each month, the same dynamic plays out in a smaller version. At the start of a woman’s cycle, a group of follicles (small fluid-filled sacs that house immature eggs) wakes up from the dormant pool and begins to grow. This group is called the recruited cohort, and in a healthy young woman, it might contain anywhere from a handful to twenty or so follicles. Not all of them are going to ovulate. They are entering a competition that evolution has been refining for hundreds of millions of years — sexual reproduction with follicle selection long predates humans — and only one is meant to win.
The mechanism that decides the winner is essentially a stress test. As the cohort begins to grow, it produces estrogen and a hormone called inhibin, both of which signal back to the brain. The brain reads those rising signals and pulls back its own output of follicle-stimulating hormone (FSH). As FSH falls, the survival threshold rises. The “dominant” follicle is not chosen by lottery, and it is not simply the biggest one; it is the follicle best able to continue growing as hormonal conditions become progressively more restrictive. The follicles that can’t keep up stall, undergo cell death, and are reabsorbed. The result is a process that selects for the follicle most capable of continuing development as conditions tighten.
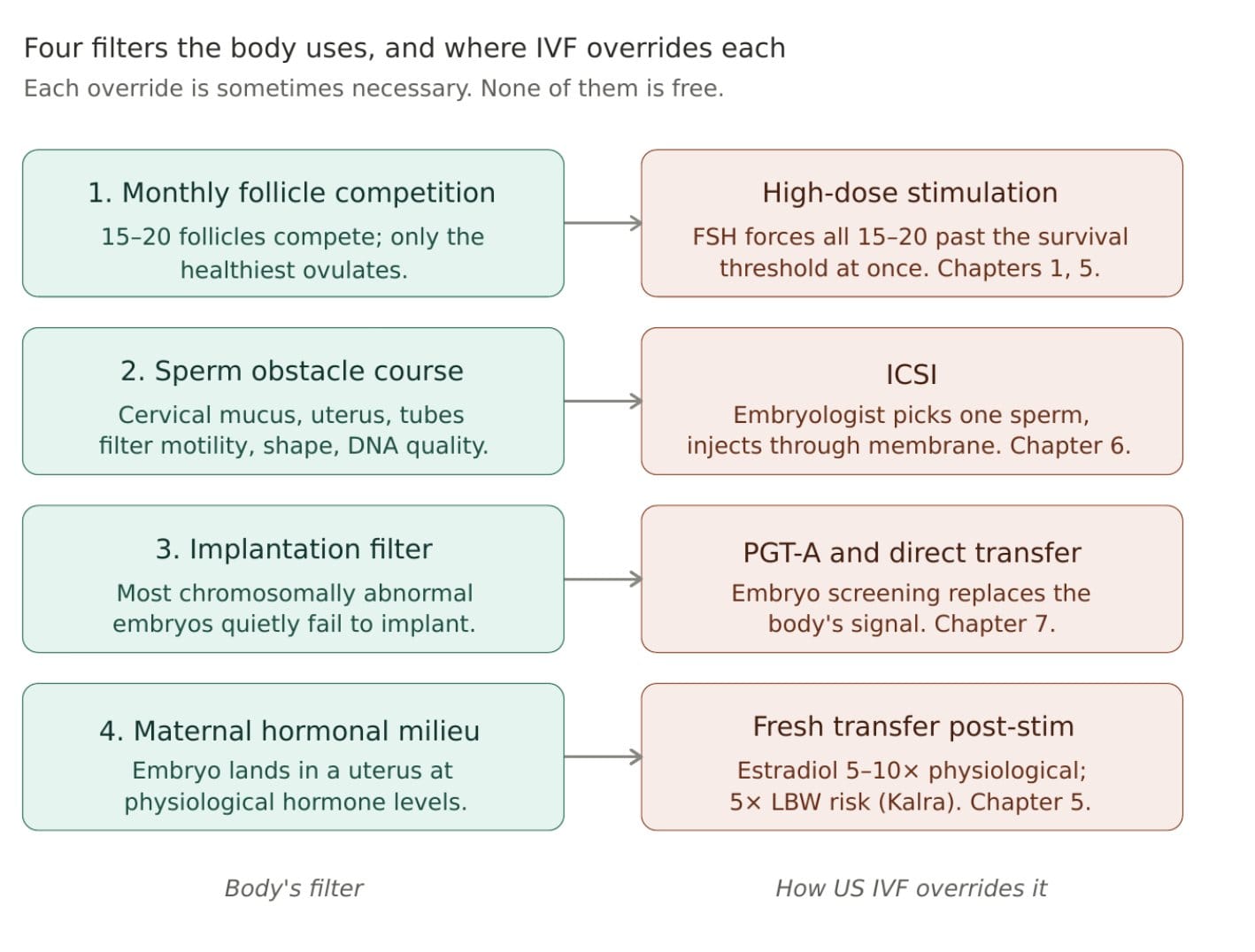
This is the part fertility medicine should probably approach with more humility than it often does. Reproduction contains multiple layers of biological selection. There are monthly competitions between follicles, the sperm-selection process within the reproductive tract, and the implantation stage, during which many chromosomally abnormal embryos fail.
Modern fertility medicine intervenes in several of these processes, often necessarily and sometimes with enormous benefit. But those interventions also alter systems that evolved to apply biological constraints and selection pressure.
IVF and egg freezing are not bad because they are unnatural — many medical interventions correctly bypass evolved processes that can produce harmful outcomes. The issue is more specific. When stimulation drugs flood the system with FSH, they short-circuit the feedback loop that normally drives follicle selection. Instead of one dominant follicle emerging from the cohort because it continued to grow under increasingly restrictive hormonal conditions, fifteen or twenty follicles are pushed past the survival threshold at once, with far less biological competition among them.
Whether that matters for the eggs ultimately retrieved, fertilized, and frozen remains an open scientific question. What we do know is that more aggressive stimulation does not reliably produce more healthy embryos. In the trial most often cited on this question, mild and conventional stimulation produced the same absolute number of chromosomally normal embryos per cycle — the conventional arm just produced more eggs overall, a higher share of which were abnormal. Larger subsequent studies have found similar patterns, with a smaller share of retrieved eggs developing into viable embryos as the total number of eggs climbs.
The egg the body would have selected in a natural cycle is the follicle that successfully passed the normal selection process. The additional follicles recruited during aggressive stimulation are follicles that ordinarily would not have continued developing that month. Fertility medicine generally treats those eggs as functionally equivalent to the naturally selected one, even though animal studies consistently find that eggs from non-dominant follicles are less likely to develop into healthy embryos — a finding whose implications for humans remain unresolved.
Chapter 1: AMH does not measure your fertility
What AMH actually measures, and why a single reading is unreliable
If you ask a doctor about your fertility, the workup will almost certainly begin with Anti-Müllerian Hormone (AMH) and an Antral Follicle Count (AFC). AMH is often presented as an indicator of how many eggs a woman has “left,” but that framing is more approximate than many patients realize. It is not a direct count of the total eggs remaining in the ovaries, and it says very little about egg quality.AMH is better understood as a snapshot of how many follicles are actively growing at that moment and, therefore, how strongly the ovaries are likely to respond to stimulation drugs. That makes it useful for IVF planning, but it does not make it a crystal ball for fertility.
The tests themselves are also less reliable than many clinics imply. Different labs use different assay methods, and there is still no fully standardised approach to AMH measurement. The practical implications matter. AMH should ideally be tracked using the same assay at the same lab over time, with careful attention to units (ng/mL versus pmol/L). Even then, levels fluctuate naturally from month to month. I saw this myself by running the experiment: my results at the same lab ranged from ‘low’ to ‘normal’ within relatively short periods.
I am not unusual in that variability. A 2024 study of 1,871 patients with repeat blood samples found that 42% of women initially classified as having low AMH later tested above the cutoff after a repeat measurement. A 2016 study found ~20% variation just across the menstrual cycle, again sufficient to reclassify 29% of participants between the “low” and “normal” categories. Another study measuring AMH repeatedly across consecutive cycles found variation as large as 446 % between the highest and lowest readings in the same woman using the same assay platform.And yet almost every fertility clinic will prescribe aggressive medical protocols based on one reading.
The Antral Follicle Count (AFC) is the more direct measurement. Performed by ultrasound at the beginning of a woman's cycle, it counts the small follicles visible in the ovaries that month, making it a better predictor of how the ovaries will respond to stimulation drugs than AMH. But results vary among technicians and ultrasound machines, and even repeat scans of the same woman can yield different results. Like AMH, AFC says nothing about egg quality - only how many follicles happened to be visible that day.
The most informative fertility workup uses AMH and AFC together, interpreted cautiously and in context. Neither test, especially in isolation, is as definitive as clinics often present it.
Even setting aside assay variation, a single day's bloodwork is often a much weaker signal than fertility clinics treat it as. I learned this the hard way. At one checkup, my hormones came back so abnormal that a doctor warned I might be in rapid ovarian decline and recommended immediate high-dose IVF. The only reason I suspected something was off was that I had recent baseline data showing a very different picture. Eventually, after reading the ingredients on everything around me, I traced the abnormalities back to a scalp serum a hairdresser had lent me — it contained estradiol.
The situation turned out to be reversible. But it revealed how easily everyday products can distort fertility panels, and how quickly abnormal numbers in a woman in her thirties can trigger escalation toward intervention before any serious investigation. Hormonal panels can be influenced by countless variables that neither clinics nor patients consistently check to identify: over-the-counter hormone products, recently discontinued hormonal contraceptives, and potentially even products with endocrine activity such as certain essential oils, parabens, and phthalates.
A clinic that does not ask and a patient who does not know to volunteer the information can end up treating a temporary hormonal snapshot as a durable biological signal.One abnormal result can quickly push a woman toward IVF or egg freezing based on what may ultimately be a reversible artefact. Retesting matters.
How AMH became a “fertility test”
AMH was originally validated for one specific job: predicting how strongly a woman’s ovaries would respond to stimulation drugs during IVF. That is a real and clinically useful use case. How it became a broad “fertility test” marketed to healthy women in their twenties and thirties is a different story.
One of the central figures in expanding AMH's role in the United States is Dr David Seifer, a Yale professor and former president of SART, the professional organisation that sets clinical and laboratory standards for US fertility clinics. The clearest illustration of the problem appears in a 2017 review paper he co-authored in the American Journal of Obstetrics and Gynecology called Ovarian Reserve Testing: A User's Guide.
The paper is interesting not because the science is wrong. It is interesting because, in the same paper recommending broader AMH use, Seifer himself holds royalties on the AMH test, and the authors repeatedly acknowledge the test's limitations.Throughout the review, the authors cite studies showing that women with extremely low or even undetectable AMH still conceived and had live births. They acknowledge published critiques arguing AMH should not be used as a fertility-planning tool in healthy women and note that ovarian reserve markers perform poorly at predicting who will actually become pregnant naturally.
And then, in the same paper, the formal indications table recommends AMH testing for women considering elective egg freezing and for estimating reproductive lifespan and menopausal timing. The paper undermines its own recommendations and the recommendations win anyway.
The strongest evidence on whether AMH predicts natural fertility refutes the way the test is now marketed. In 2017, a JAMA study followed 750 women aged 30 to 44 with no history of infertility who had just started trying to conceive, exactly the population AMH is now sold to. Low AMH was not associated with a lower probability of conceiving within twelve cycles. High FSH did not predict who became pregnant naturally either.
The study has limits — it followed women for only one year, and the subgroup of women aged 38 to 44 with low AMH was small. But it directly undermines the much broader consumer claim now attached to AMH testing: that a single AMH reading tells a healthy thirty-something woman something meaningful about her near-term ability to get pregnant. It does not. AMH genuinely predicts ovarian response to stimulation drugs. That is the use case it was validated for. The problem is that it is now widely sold as a broader fertility predictor even though the evidence supporting that expansion is much weaker.
Once that shift happens, the commercial logic becomes straightforward. AMH becomes part of the routine “fertility evaluation.” A healthy woman in her early or mid-thirties is told she may have a narrowing reproductive window. Egg freezing becomes the natural next recommendation. Egg freezing requires stimulation drugs dosed using AMH. Retrieval leads to storage fees, thaw cycles, and often IVF.AMH sits near the top of a commercial pathway that can turn reproductive anxiety into years of downstream fertility treatment.
How aggressively this is marketed in the US, compared to other countries
AMH testing in the US looks almost nothing like AMH testing in the rest of the developed world. Here, it’s sold direct-to-consumer by venture-backed startups, branded as the “egg timer” or “biological clock test,” and offered as a pop-up service in trendy neighbourhoods. In most other countries, it’s a clinical tool used inside a fertility consultation when an actual treatment decision is on the table.
A 2023 JAMA Network Open analysis of websites selling AMH tests direct to consumers found that 96% claimed the test indicates ovarian reserve, 74% claimed it indicates the likelihood of conceiving, 41% encouraged women to use the result to “adjust their reproductive timeline,” and 30% promoted it as a way to decide whether to freeze eggs. Most leaned on language about convenience, empowerment, and control; only a third disclosed that the test cannot actually predict the chance of conceiving. The authors concluded that most of the sites contained false or misleading claims.
The US is the extreme version. Modern Fertility (acquired by Ro for $225m in 2021) ships finger-prick kits that women feed into proprietary “fertility scores.” Kindbody runs branded mobile clinics, “fertility buses”, offering free AMH tests as feeders into its egg-freezing service, a strategy its founders modelled on SoulCycle and Drybar. One expert in 2018 called the marketing “a scare tactic in the guise of information”. The underlying message is always: know your fertility before it’s too late. The brands, the pop-up clinics, the Instagram aesthetic, the empowerment language, the venture funding, this whole category is American in a way that’s hard to overstate.
Other countries have moved in the opposite direction. The American College of Obstetricians and Gynecologists itself discourages AMH testing in otherwise healthy women, a position the US fertility startup ecosystem ignores. The UK’s NHS does not routinely offer AMH to women curious about their fertility; it’s measured inside a clinic when a treatment decision is being considered, not sold as a planning tool.
The defensible uses of AMH are predicting ovarian response to stimulation drugs, dosing those drugs in IVF, and supporting a PCOS diagnosis. Everything beyond that, telling a woman her fertility window, guiding egg-freezing decisions, “biological clock” testing, is overreach.
Chapter 2: Before you start any cycle, fix what’s upstream
If you walk into a US fertility clinic with a low AMH or trouble conceiving, the consultation will move within an hour or two toward a treatment plan: AMH measurement, ultrasound, talk of stimulation protocols, supplements added on, and a recommendation to start a cycle within months. What that consultation will rarely include is a thorough investigation into what might be wrong with the underlying biology that produces the fertility problem in the first place.
That something further upstream might be producing the signal, and that fixing the upstream issue might do more than any downstream intervention, is essentially absent from standard clinical workflow. This is a strange omission because fertility is one of the most metabolically expensive functions a body performs, and it shuts it down quickly when other systems are stressed.
The logic makes sense evolutionarily- getting pregnant during a famine, an illness, or a period of extreme stress would have been catastrophic for our ancestors, so the body evolved to pause reproduction whenever conditions look bad. That pause is real, and it happens fast.The control centre for this is the hypothalamus. a region in the brain that runs the entire reproductive cascade through timed pulses of a hormone called GnRH.
GnRH tells the pituitary gland to release the hormones that drive your ovaries, which in turn produce estrogen and trigger ovulation. The hypothalamus sits inches away from the regions that monitor sleep, stress, body temperature, blood sugar, and energy availability, and it uses overlapping hormonal pathways with these regions.
When any of those upstream systems is out of balance (too little sleep, too much cortisol, too few calories, too much exercise) the GnRH pulse generator slows down, estrogen drops, and ovulation becomes irregular or stops altogether. The clinical name for the extreme version of this is functional hypothalamic amenorrhea, and it accounts for a meaningful share of women who present at fertility clinics with “unexplained” infertility.Reviews of low energy availability in women suggest the subtler effects often appear well before menstruation stops entirely: weaker ovulation, shorter luteal phases, and reduced fertility. Even a fairly modest persistent calorie deficit can disrupt the hormonal signals that regulate ovulation.A long-running calorie deficit, intentional or not, is metabolic information the brain reads as “not a good time to make a baby.” The clinical recommendation in the actual literature is to eat more, not to stimulate harder.
None of this is fringe- it is the mechanism described in every reproductive endocrinology textbook. It is just not the framing American fertility clinics use, because it leads to recommendations (sleep more, eat more, train less, lower stress) that aren't easy to market.
Furthermore, the body has two main stress systems- one is the cortisol pathway (the “HPA axis”), which is the slower, hormonal stress response. It’s the system that ramps up when you’re under sustained psychological pressure. The other is the sympathetic nervous system, which is the faster “fight or flight” response, racing heart, shallow breath, the wired feeling of being constantly on. A common saliva test, alpha-amylase, measures activity in the second system.
The LIFE study, followed a cohort of 501 couples trying to conceive, found that women with the highest alpha-amylase levels had a 29% reduction in their chance of conceiving each cycle, and roughly double the risk of being diagnosed with clinical infertility, compared to women with the lowest levels. The Oxford Conception Study found a similar association.
The interesting detail in both studies is that alpha-amylase tracked with infertility, but salivary cortisol did not. The “stress affects fertility” story isn’t really about feeling worried or anxious in the conventional sense; it’s about chronic activation of the fight-or-flight system, the kind that comes from poor sleep, overwork, undereating, overtraining, and never genuinely settling.
Hair-cortisol studies which measure chronic cortisol exposure over months rather than momentary stress, show a more mixed but potentially more meaningful signal. In some IVF cohorts, elevated hair cortisol predicted lower pregnancy rates even when salivary cortisol did notNone of this proves that stress alone causes infertility. But it does mean that “have you actually slept properly in the last two years?” is a question that should be asked before a stimulation protocol is started, and almost never is.
A meta-analysis of more than 119,000 women found that night-shift workers had a 33% higher rate of menstrual disruption, along with elevated rates of miscarriage and subfertility. A larger 2023 meta-analysis covering ~ 196,000 female night-shift workers confirmed the menstrual-irregularity finding and added a small but real association with earlier menopause.The strongest data is on shift workers, specifically because they’re the easiest group to study, because their disruption is extreme and well-documented. But the same biological pathway is being tugged on by anyone who routinely sleeps four or five hours, anyone whose sleep timing varies by more than two hours from one night to the next, and anyone who scrolls on a bright phone at midnight. That’s most knowledge workers in San Francisco or New York.
Sleep, chronic stress, energy availability, thyroid dysfunction, insulin resistance, iron deficiency, endometriosis, uterine pathology, chronic inflammation, and male-factor issues can all influence fertility in ways that standard IVF-centered workups do not always explore particularly deeply before escalating toward intervention. Many are relatively common, measurable, and in certain cases reversible. One study, for example, found chronic endometritis, a low-grade uterine inflammation that often produces no obvious symptoms, in over half of women with unexplained infertility.
Infertility can't always be solved through lifestyle changes or upstream optimisation. Many cases genuinely require IVF, and for many people, IVF is an extraordinary technology. But the current American workflow often leans toward ovarian stimulation before upstream contributors have been systematically investigated, even when the literature itself supports seeking them.
The value of tracking your own cycle hormonally
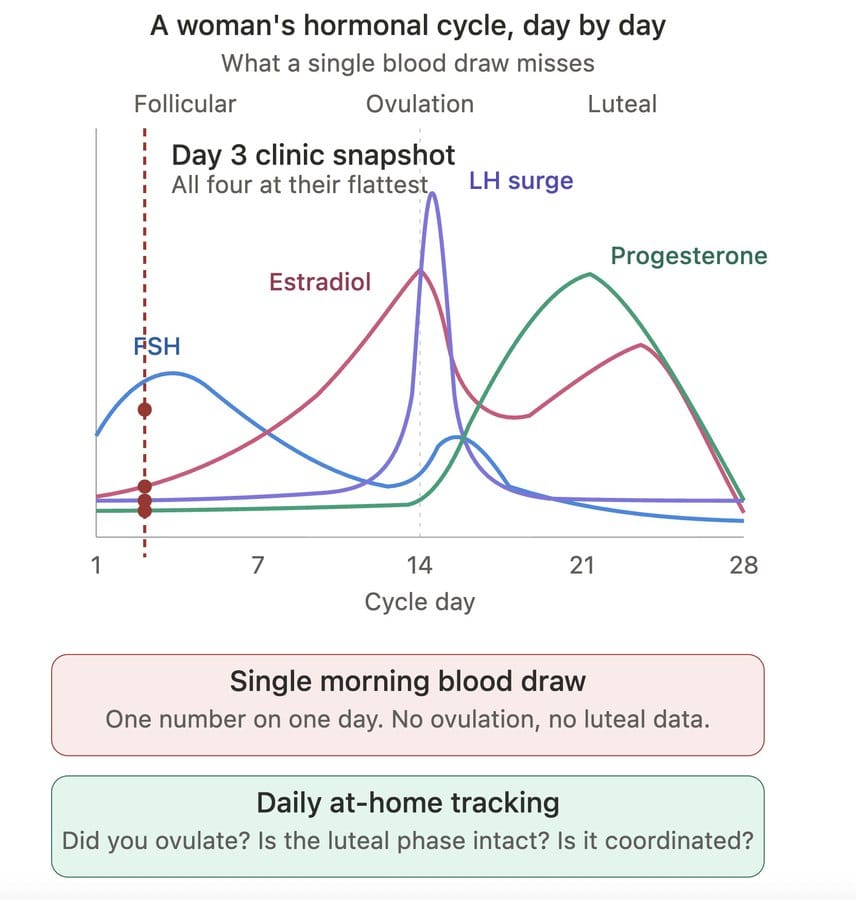
A separate step alongside all of the above is to track your own cycle for a few months before any clinic appointment. Devices like Inito and Mira measure estrogen, LH, FSH, and progesterone metabolites from daily urine samples at home and chart your cycle. They are not substitutes for clinic-grade blood work, and the evidence base around at-home hormone monitoring is still developing. But what these devices are genuinely useful for is something standard fertility workups can't easily provide: a longitudinal view of your own hormonal patterns over time, rather than a snapshot from a single morning blood draw.
The underlying cycle biology is well established, and urinary hormones track closely enough during natural cycles to indicate whether ovulation is occurring and whether the hormonal sequence across the cycle functions in a coordinated way. These kinds of patterns are difficult to infer from a single day-3 FSH, AMH, or estradiol blood panel done by a clinic.
I started doing this early in my own research, screenshotting the readouts and asking AI systems to help me interpret the patterns, until the shape of my own hormonal rhythm became legible to me. This changed the dynamic in a meaningful way. Instead of encountering my fertility only as a series of isolated lab values interpreted by someone else, I had already begun to develop a working picture of how my own cycle behaved over time.
Chapter 3: The egg-freezing insurance premium is more expensive than it looks
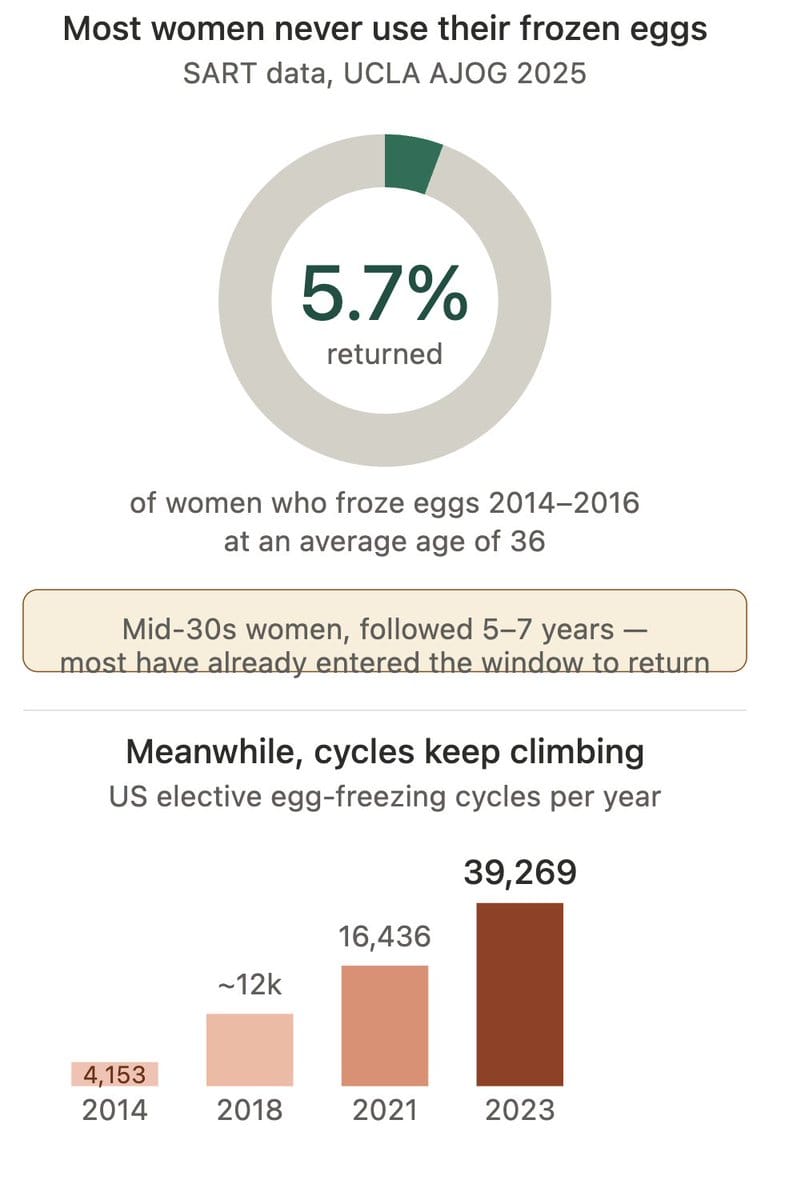
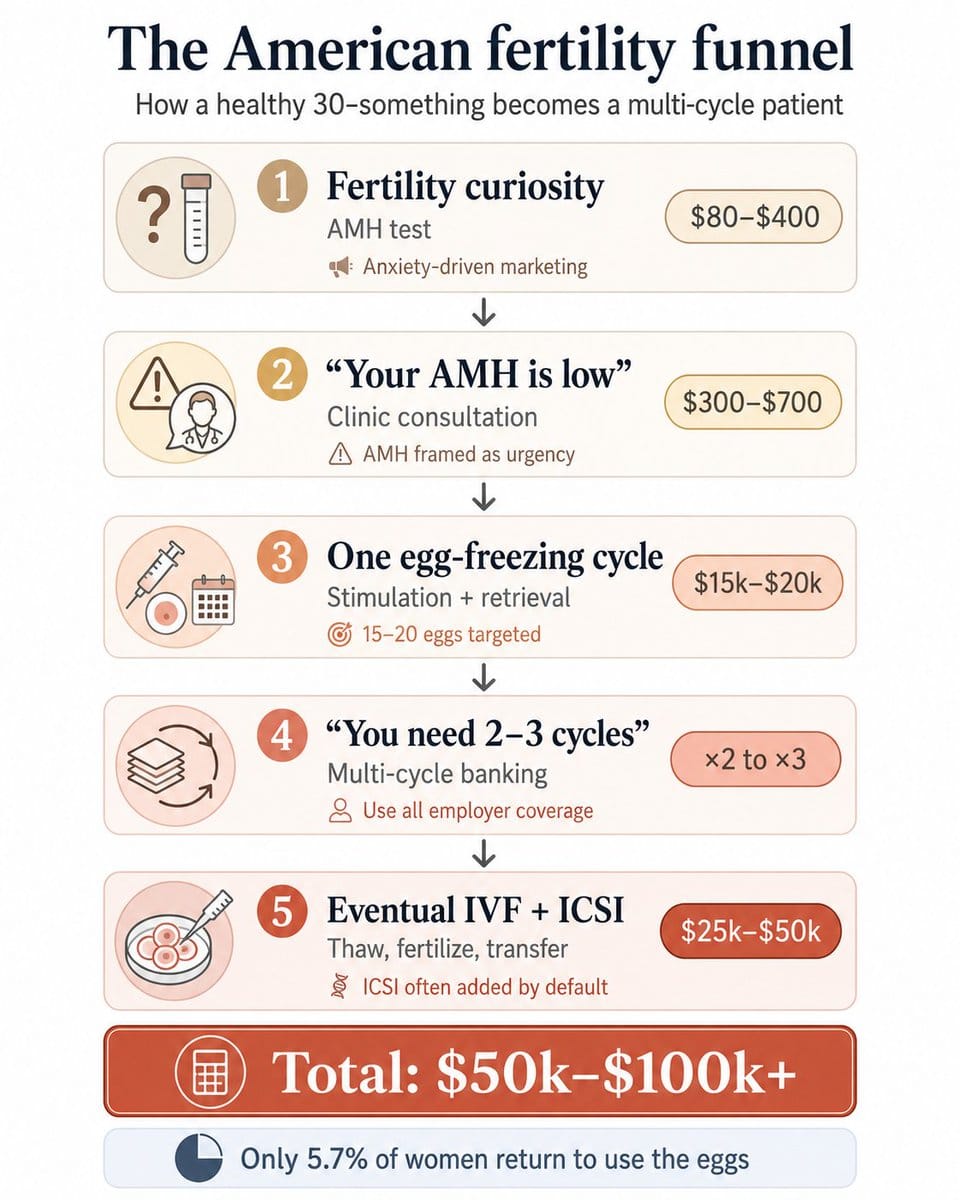
The most reliable picture of the rise of US elective egg freezing comes from a 2025 UCLA study published in the American Journal of Obstetrics and Gynecology, which used the SART database, the largest and most complete record of US fertility cycles. It found that elective egg freezing nearly quadrupled between 2014 and 2021. Of women in their mid-thirties who froze their eggs between 2014 and 2016, only 5.7% returned to use them within a 5- to 7-year follow-up window.
The 5.7% return rate is sometimes cited as evidence that the industry is exploitative. That framing is wrong because egg freezing is sold as insurance, and most insurance policies don’t pay out. The financial premium, roughly $15,000–$20,000 per cycle plus annual storage, is disclosed clearly. But other premiums aren’t.
The first underdisclosed cost is that one cycle usually isn’t enough. A single retrieval at age 35 typically yields 10–15 eggs, of which perhaps half will survive the thaw and fertilise, and of which perhaps half again will become viable embryos. To bank a meaningful insurance policy, say, the rough equivalent of two future pregnancy attempts, most women under standard US protocols need two or three cycles. Each one is its own round of injections, monitoring, retrieval, and recovery.
The “freeze your eggs” pitch quietly slides into “freeze your eggs, then freeze them again, and possibly again.” Clinics quote per-cycle pricing; the actual cost of a real insurance policy is some multiple of that.
The second underdisclosed cost is the endocrine exposure itself. The risks discussed at consent are almost entirely acute and procedural: ovarian hyperstimulation syndrome (OHSS), occurring in roughly 3–6% of cycles overall and in less than 1% in severe form; bleeding, infection, or ovarian torsion at retrieval, with torsion rare in routine retrievals but rising to around 2% among hospitalized OHSS cases. These are real and happened to my friend, but they are also easy to disclose. They are also largely a function of stimulation intensity — milder protocols cut OHSS risk by roughly half to three-quarters in randomised trials, with no loss in live birth rates. The cumulative endocrine exposure doesn't get the same attention: pushing estradiol levels to superphysiological levels for 10 to 14 days, repeated across multiple cycles, in women whose long-term hormonal exposure profile matters for outcomes that show up decades later.
Chapter 4: You probably do not need all those shots
What’s actually in an American IVF cycle in 2026
From the body’s perspective, “IVF,” “egg freezing,” and “embryo banking” are not three wholly different procedures. They share the same upstream intervention: the stimulation protocol, the daily medications, the cumulative hormone load, the trigger shot, and the retrieval surgery. What differs is what happens after retrieval.
A typical American cycle today involves an extraordinary cocktail of hormonal medications layered on top of one another over roughly a month, with the system structured around retrieving as many eggs as possible per cycle.Women often begin with birth control pills to synchronize the cycle, then transition to 10–12 days of daily injectable gonadotropins (FSH), often combined with luteinizing hormone (LH), under brand names like Gonal-F, Follistim and Menopur, to force the ovaries to develop 15–20 follicles simultaneously rather than the single follicle a natural cycle produces.
After completing the stimulation, women receive one last injection of medication- a “trigger shot” that forces the eggs to complete maturation so they can be retrieved on a precise schedule ~36 hours later. This medication load has escalated dramatically since IVF began in the US in 1981. Early IVF protocols used minimal stimulation and targeted 2–4 eggs per cycle. Through the 1990s and 2000s, doses climbed as clinics competed on success rates.
By the 2010s, after the “experimental” label was removed from egg freezing in 2012, high-dose protocols targeting 15–20 eggs per cycle became the US standard. The trajectory is unambiguously upward: more drugs at higher doses and longer protocols, and increasingly multi-cycle regimens as women are encouraged to bank twenty or more eggs.
The rationale for aggressive stimulation is the same one used to justify almost every intensification in American medicine: do as much as possible per visit. IVF is physically, emotionally, and financially burdensome, so clinicians and patients prefer maximising eggs retrieved per cycle in the hope of minimising the number of retrievals required. Fewer retrievals, the logic goes, must mean less suffering and less drugs overall. This is the assumption that does the most work in the conversation between American fertility doctors and their patients, and it is the assumption that turns out, when you look closely, to be wrong.
The rest of the world does this differently
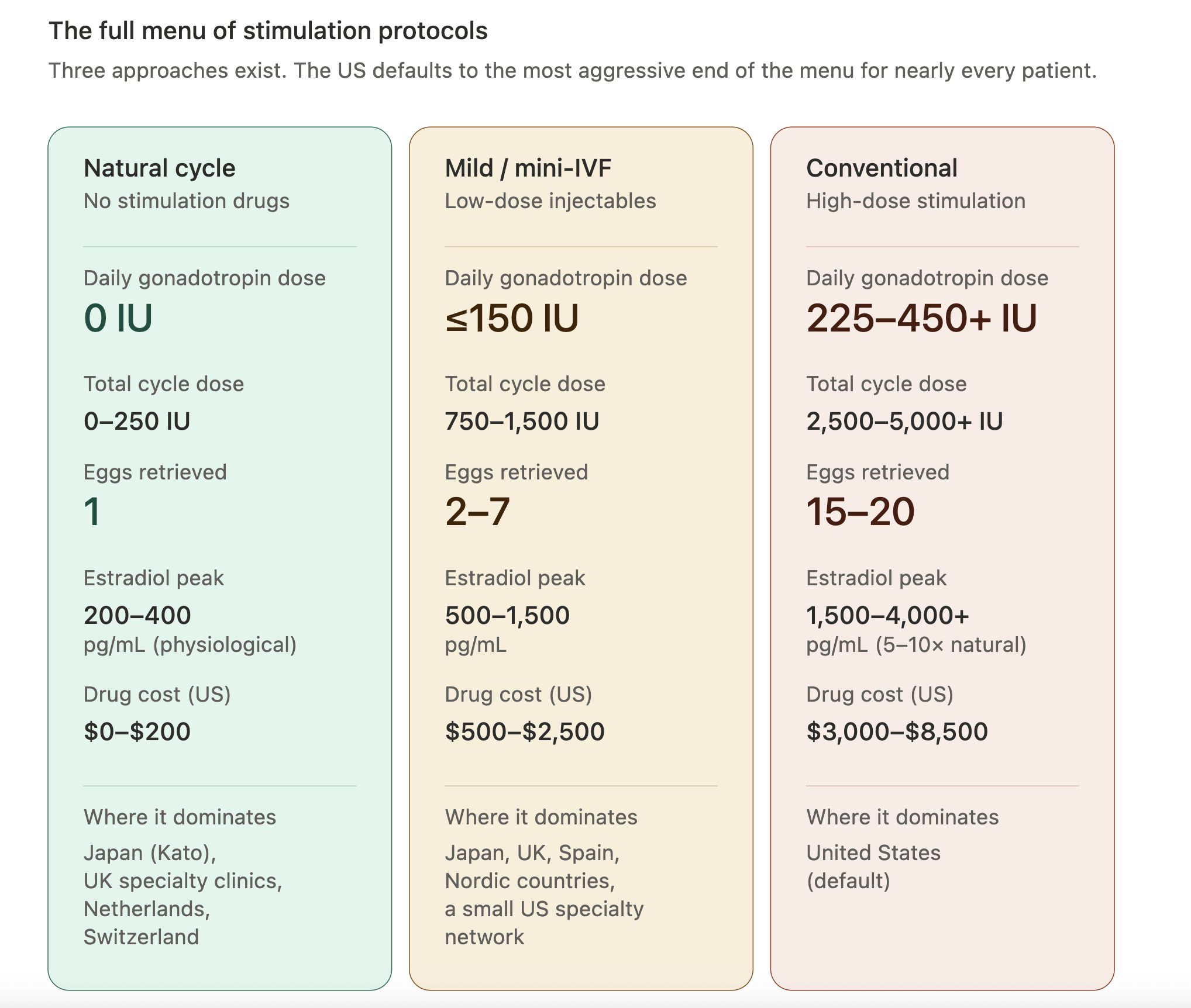
The intensity of medication exposure in US egg freezing is not a universal feature of fertility medicine. It is an American phenomenon, driven by US-specific commercial, regulatory, and cultural forces. Other countries with developed reproductive medicine systems use the full menu of options, natural cycle, mild, moderate, and conventional protocols, and reach for the most aggressive option much less readily. The US, by contrast, defaults to the most aggressive plan for nearly every woman who walks in the door.
Three distinct approaches exist along this menu, and the difference between them is not just the dose; it is a fundamentally different theory of what an IVF cycle is for. “Natural-cycle IVF” and “mild-stimulation IVF” take a very different approach from the high-dose protocols common in the United States. Instead of trying to recruit the largest possible cohort of follicles, these approaches aim to work more closely with the body’s existing cycle and retrieve a smaller number of eggs with substantially lower hormone exposure.
Natural-cycle IVF typically retrieves the single dominant follicle the body was already preparing to ovulate, sometimes timed with a trigger such as buserelin nasal spray. Mild IVF adds lower-dose stimulation medications, often alongside oral agents like clomiphene or letrozole, with the goal of retrieving a small cohort of eggs rather than maximising yield.
The best-known center associated with this philosophy is the Kato Ladies Clinic in Tokyo, which has specialized in natural-cycle and minimal-stimulation IVF since the 1990s and performs tens of thousands of retrievals per year. Similar approaches are common across Japan and available throughout parts of Europe, but remain relatively uncommon in the United States.
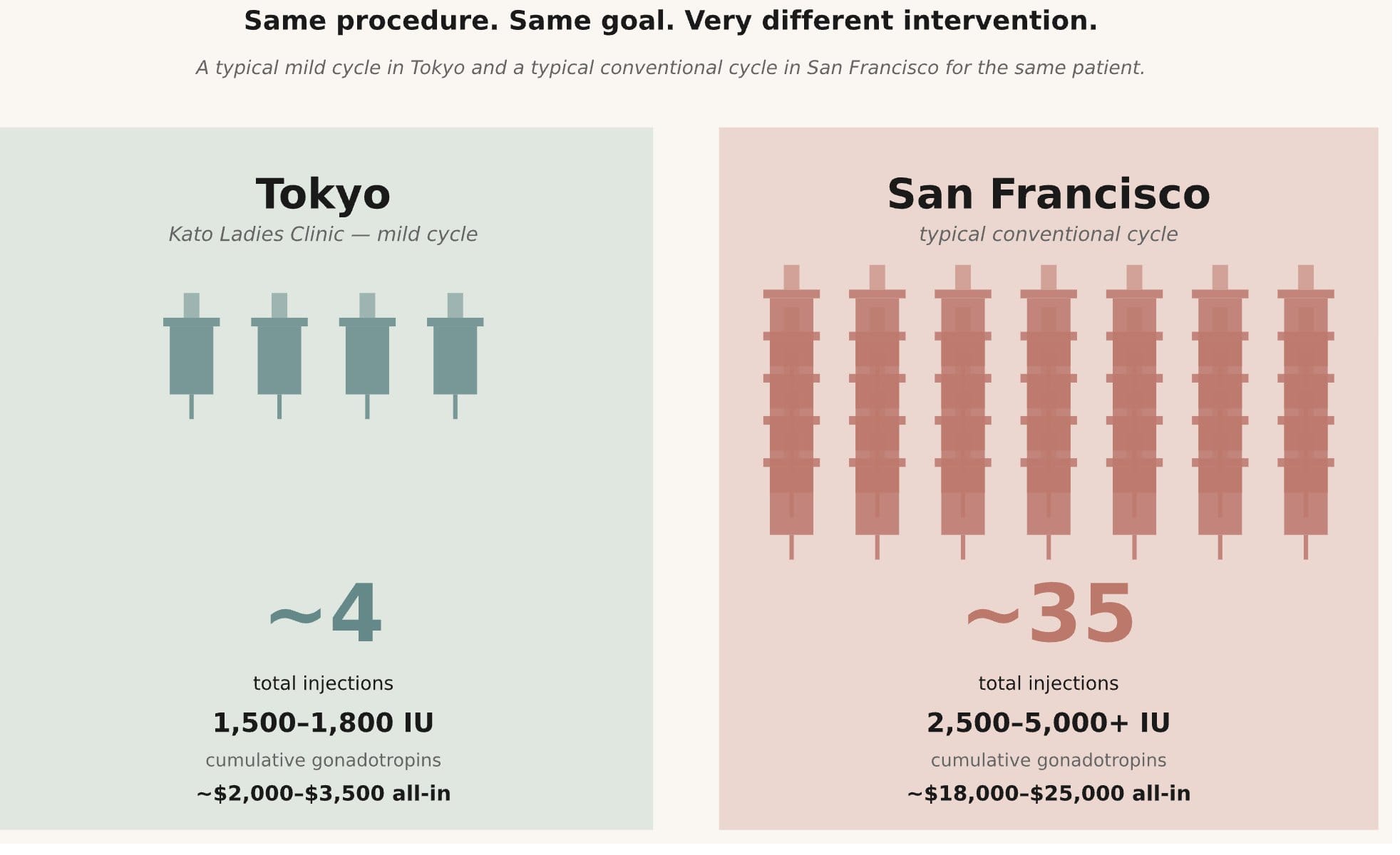
Conventional high-dose IVF is the protocol that dominates American elective egg freezing. Daily injectable gonadotropins commonly run 225–450 IU, sometimes higher, for around 10–12 days, with the goal of retrieving the largest possible cohort of eggs in a single cycle. Many protocols also begin with weeks of hormonal suppression before stimulation even starts, and additional hormone adjuncts such as growth hormone, DHEA and testosterone.
This is the version of IVF most American women encounter, mostly without being told there are materially different stimulation philosophies elsewhere. The difference is not just pharmacological but philosophical. Natural-cycle and mild-stimulation clinics accept fewer eggs per retrieval in exchange for dramatically lower hormone exposure, often a fraction of what women receive in conventional American protocols.
Because the cycles are physically easier and closer to physiological hormone levels, patients can repeat them multiple times with less disruption and cumulative exposure rather than trying to extract the maximum possible number of eggs in a single aggressive cycle.
Underneath that is a different view of what fertility medicine looks like. The goal is not to overpower the ovaries into producing the largest possible cohort, but to work more closely with the body’s existing selection process and intervene as lightly as possible while still achieving pregnancy.
The outcome data doesn’t even justify the extra medication
The intuitive case for high-dose stimulation is simple. More eggs mean more chances at fertilisation, more chances at a healthy embryo, and therefore more chances at a baby, either immediately or later out of the freezer. If a clinic can retrieve fifteen or twenty eggs instead of five, that sounds obviously better. Nearly every American woman walking into a fertility consultation absorbs some version of this logic.
But once you look at the actual dose-response literature, the picture becomes more complicated.Some of the clearest evidence comes from trials that directly randomized women to different stimulation intensities. The 2007 Heijnen trial randomized 404 women to mild versus conventional IVF stimulation and found similar cumulative pregnancy rates over one year, despite substantially lower drug exposure in the mild cohort, along with lower complications, costs and better reported quality of life. More than a decade later, the OPTIMIST trial randomized predicted poor responders to either 150 IU or 450 IU of daily FSH. The higher-dose group produced more eggs, but not more live births.
These studies do not prove that aggressive stimulation is never useful. But they do challenge one of the widespread assumptions in modern fertility medicine- that women with declining ovarian reserve necessarily benefit from escalating gonadotropin dose.
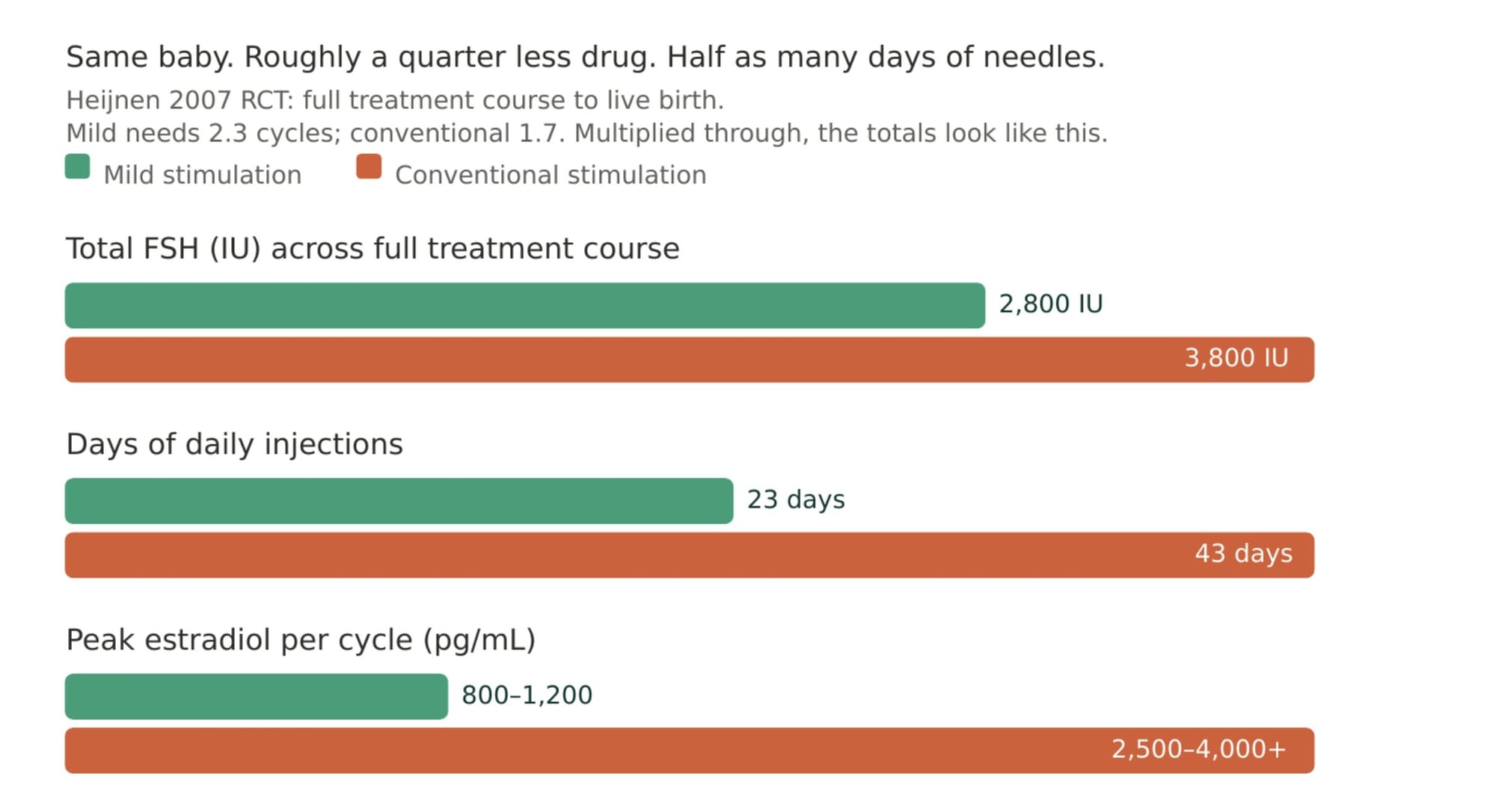
In poor responders, especially, retrieving more eggs has not consistently translated into more live births.The standard objection to mild stimulation is that women may need more retrieval cycles to reach the same goals. In the Heijnen trial, the difference was real but modest: women in the mild-stimulation arm averaged roughly 2.3 cycles compared to 1.7 in the aggressive Even accounting for the extra cycles, however, total hormonal exposure remained substantially lower in the mild group.The mild approach was easier on the body, easier on the budget, and ultimately produced the same number of healthy babies. “More cycles” sounds more like a downside if you’re accustomed to conventional IVF doses and all the side effects and stress that come with it.
Conventional US doses push estradiol to peaks of 2,500–4,000 pg/mL sustained over 5–7 days. A mild cycle peaks at 800–1,200 pg/mL, sustained over 3–4 days. Even after the extra mild cycle, total estradiol-days of exposure across the full treatment course are two to three times higher in the conventional arm.
Retrospective data points in the same direction at much larger scale. A SART analysis of more than 650,000 IVF cycles found that higher gonadotropin doses correlated with lower live birth rates, including in some good-prognosis patients. Other large observational studies in both Western and Asian populations have reported similar non-linear patterns: beyond a certain point, escalating FSH dose produces more eggs without clearly improving live birth outcomes.
A careful reader will notice the obvious objection: women receiving the highest doses are often the women predicted to respond poorly in the first place. This is a real limitation of retrospective data. But it is also exactly why the OPTIMIST randomized trial matters. It specifically tested whether poor responders benefited from dramatically higher FSH dosing and found that while the higher-dose group produced more eggs, they did not produce more babies.
None of this proves high-dose stimulation is always wrong. But it does weaken one of the central assumptions driving modern elective egg freezing: that more aggressive stimulation reliably improves the outcomes patients actually care about most.
Chapter 5: More eggs ≠ better
More eggs do generally mean more chances at fertilization and embryo development, but only up to a point. But the question is whether pushing stimulation harder keeps improving the outcome patients actually care about most- a healthy baby
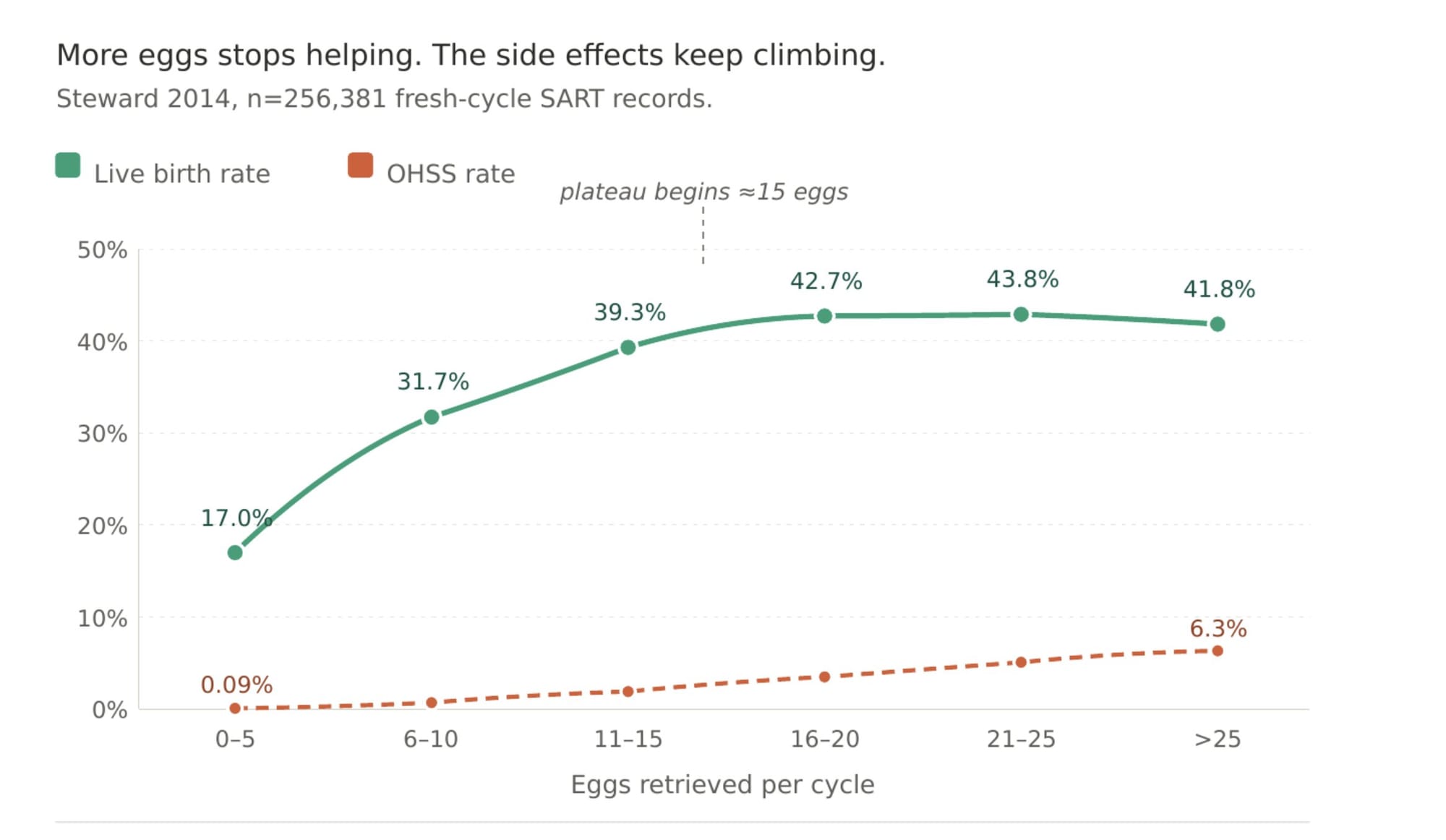
The evidence suggests the benefit is not linear. Large registry studies find that live birth rates rise as egg yield increases, then plateau around the mid-teens, while serious risks such as OHSS continue rising. A major UK analysis of more than 400,000 IVF cycles found live birth rates increased up to roughly 15 eggs retrieved, plateaued between 15 and 20, and declined beyond that point. A large US SART analysis of 256,381 IVF cycles similarly found that live birth rates barely improved beyond 15–20 eggs while OHSS risk increased sharply.
The debate is not whether more eggs can sometimes improve cumulative odds. It is about whether increasing from 12 eggs to 20 eggs is worth the additional hormonal exposure, monitoring, costs, and repeat stimulation required to get there. This matters because the “20 eggs” benchmark is often presented to women as though it were a universal biological threshold rather than one strategy among several.
The strongest egg-freezing success statistics usually come from younger women who froze earlier, produced large egg cohorts, and later returned to use them. Those numbers are real, but they are not necessarily representative of the average woman entering an egg-freezing consultation.
The “poor responder” argument is also less straightforward than it sounds. A woman with mildly reduced reserve and a woman over 40 with severe diminished ovarian reserve are often grouped together, but they are not the same patient. The OPTIMIST trial directly tested whether predicted poor responders benefited from 450 IU rather than 150 IU of daily FSH. The higher-dose group produced more eggs, but not more live births overall. That does not prove that high-dose stimulation never helps an individual patient. It does suggest that routinely escalating everyone in this category to very high doses may produce more ovarian response without clearly improving the outcome patients ultimately care about most, having a baby.
While I was working on this research, Works in Progress published an essay arguing that more women should consider elective egg freezing and recommending a target of roughly twenty frozen eggs. The piece was widely circulated, and I agree with significant parts of it.They are right that older media coverage often understated how much vitrification improved egg-freezing outcomes. They are right that freezing age matters enormously, and that many pessimistic statistics come from cohorts who froze relatively late. They are also right that some European clinics, particularly in Spain, offer technically excellent IVF at far lower cost than in the United States.What I disagreed with was not the existence of the technology but the confidence surrounding the recommendation itself, particularly the implied certainty around the “freeze twenty eggs” benchmark
The central question addressed by the WIP authors was “Should women freeze their eggs?” The technology itself is real, and it helps people. But perhaps the more important question is why the most medically aggressive version of the process has become treated as the obvious default and not questioned, even by the authors.
I do think this kind of high-confidence messaging can have consequences. A friend in San Francisco recently overheard a young woman telling friends over brunch that she was secretly taking more of her egg-freezing medication to try to generate “20 eggs.” That is only an anecdote, but it captures the danger of turning a flimsy statistical target into a cultural command.
The cultural pull toward intensity
More shots, higher doses, longer protocols, and larger egg counts create the feeling that everything possible is being done. But intensity and effectiveness are not always the same thing. This pattern reflects a broader cultural instinct toward continuous optimization and intervention, the belief that if some intervention is good, more must be better. Fertility medicine mirrors the rest of American wellness culture in this way.
Women post their injection counts and bruised stomachs on Instagram stories, almost like endurance badges, proof of commitment and seriousness, not unlike the way men in biohacking circles list peptide stacks or testosterone protocols. I do not think most women are consciously glamorising suffering. But I do think the culture around fertility treatment has started to normalise a level of medical intensity that would have felt extreme not very long ago.
What is being sold to healthy women is not a wellness optimisation. It is a month-long endocrine intervention involving dozens of injections, supraphysiologic hormone exposure, surgery under sedation, and real biological uncertainty.
Chapter 6: What we still don't know about long-term hormonal exposure
The honest answer about modern fertility drug exposure and long-term risk is that we do not know as much as patients are often led to believe., published in 2024, concludes that available data does not show an association between fertility drugs and breast, colon, or cervical cancer — but acknowledges there may be increased risks of invasive and borderline ovarian cancers, and of thyroid cancer. The position is not that fertility drugs are risk-free. It is that the evidence is not yet strong enough to establish a clear causal relationship for most cancers.
The American Society for Reproductive Medicine's most recent practice guideline on fertility drugs and cancerfound that women with a family history of breast cancer who underwent fertility treatment had roughly 35% higher odds of developing breast cancer than similar women who didn't. The result was borderline — it didn't quite clear the standard threshold for being unlikely due to chance, but it crossed that threshold once a few weaker studies were removed. The reviewers themselves flagged serious quality problems with most of the underlying studies, and concluded it was 'hard to confirm the safety of fertility treatments in women with a family history of breast cancer.'
The picture is shakier when you look specifically at women with a higher genetic risk of breast cancer - those with BRCA mutations or close relatives who've had it. A2022 review pooling multiple studiesof more than 250,000 British women found that the more IVF cycles a woman went through, the higher her risk of an early-stage breast cancer that hadn't yet spread — women with five or more cycles had over twice the expected rate. Fully invasive breast cancer was not elevated, but the women had only been followed for an average of about nine years.
The study also found higher ovarian cancer rates, which the authors mostly chalked up to other factors common in IVF patients — like endometriosis or never having been pregnant — rather than the drugs themselves, while admitting they couldn't fully separate the two. The authors flagged that the early-stage breast cancer signal looked causal because the risk rose with the number of cycles, though they couldn't rule out that women undergoing IVF were perhaps just being screened more often.
Even some of the largest studies cited as evidence of safety become more complicated when you read them closely. A2018 BMJ study, found no overall increase in breast cancer risk after IVF. But those women were treated between 1983 and 1995, and the authors themselves admitted the findings may not apply today. The drugs, the doses (much lower back then), the number of cycles, and the kinds of women undergoing IVF have all changed a lot since then.
Another study often cited as reassuring,a Dutch cohort followed for over 20 yearsNone of this proves that fertility drugs cause cancer. But it does mean the evidence is more uncertain, population-specific, and protocol-dependent than the simplified "no association" summary often given to patients.
The most important issue for women reading this today is that the follow-up periods in the reassuring studies are still relatively short compared to the biology of the diseases they are trying to rule out. Hormone-sensitive breast cancers often take decades to develop, with peak incidence in the late 60s and 70s. A woman who froze her eggs in her 30s will not pass through the highest-risk age window for another thirty or forty years. The largest reassuring IVF studies generally follow patients for roughly 9 to 21 years, not the 30-plus years that would fully capture late-developing risk. And the cohorts with the longest follow-up are the ones treated with older, lower-intensity protocols — not the high-dose, multi-cycle regimens now common in American elective egg freezing.
The cohorts with the right exposure profile haven't been followed long enough; the cohorts with long-enough follow-up had a different exposure profile.
History gives some reason for caution about hormone-related risks that take decades to show up.DES, a synthetic estrogen prescribed to an estimated two to four million pregnant women between the 1940s and 1970s, was approved on weak evidence and heavily marketed to prevent miscarriage.A 1953 randomised trialfound it had no effect on miscarriage at all — yet the drug stayed in widespread use for nearly two more decades, untila 1971 paperlinked exposure in the womb to a rare vaginal cancer in young women. The daughters of women given DES turned out to have roughly 40 times the normal riskof that cancer, and the mothers themselves had a higher risk of breast cancer in some studies- one of the largest harm-from-medicine episodes of the era.
The eventual fix was simple- adding a second hormone, progestin, largely eliminated the uterine cancer risk — but it took decades to be figured out and made standard. A second example is estrogen given to women after menopause. Hormone replacement was introduced in the 1940s and prescribed widely through the 1960s and early 1970s on the assumption that it was safe. Then, in December 1975,two studiesreported that women taking estrogen alone had four to eight times the normal rate of uterine cancer, with risk rising further the longer they took it. Estrogen replacement is now thought to have causedaround 15,000 extra cases of uterine cancer in the U.S. between 1971 and 1975 alone
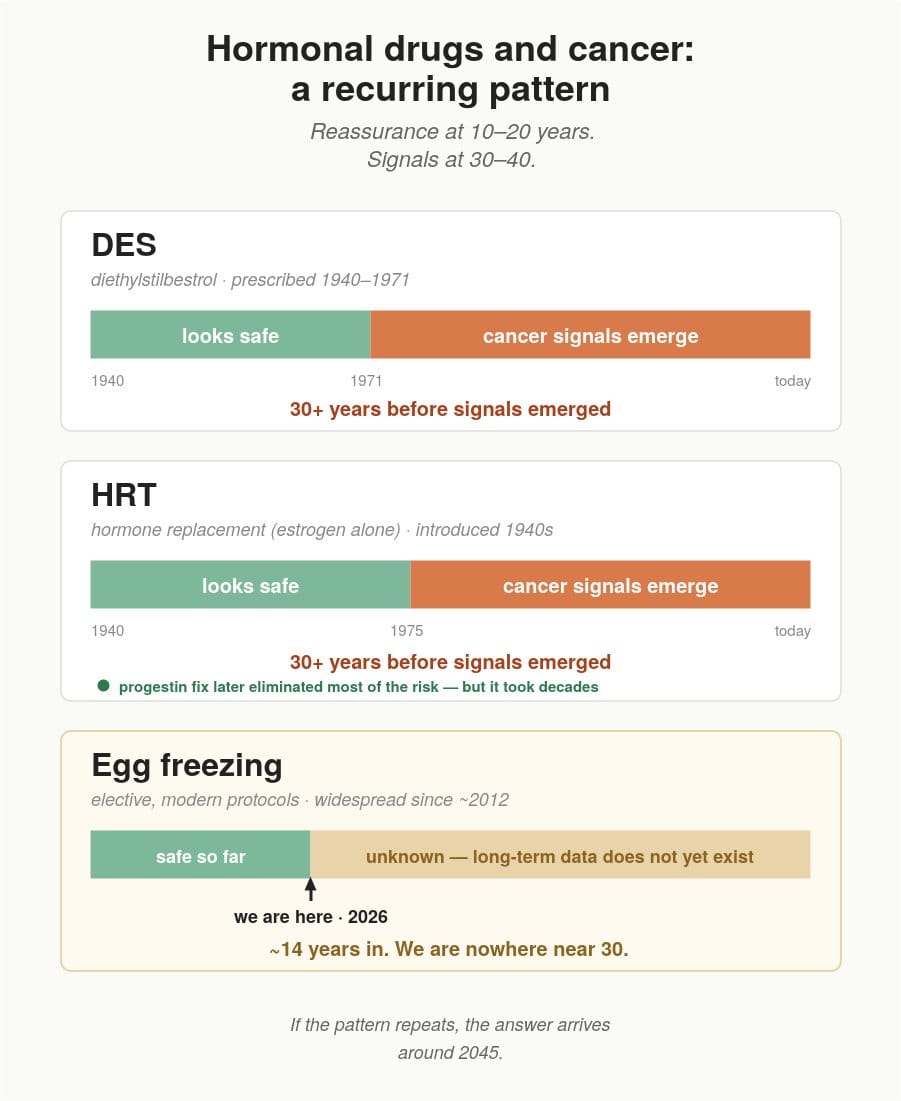
These histories don't mean fertility drugs belong in the same risk category. The biological contexts differ, and the exposures in IVF are much shorter. But they do illustrate that large-scale hormonal interventions can remain uncertain for decades while medium-term data look fine, and that "no signal at year ten" has historically meant "wait twenty more years" more often than the field is comfortable admitting.
That gap matters especially for modern elective egg freezing. The "experimental" label was removed only in 2012, and widespread adoption accelerated primarily after 2015. The women exposed to today's high-dose elective-freezing protocols have at most about a decade of follow-up. Meanwhile, the older studies most commonly cited as reassuring largely involve 1980s and 1990s IVF patients who underwent fewer cycles and substantially different protocols than many modern elective freezers.
It's worth being precise about what "small absolute risk" actually means at scale. An extra 1.7 in situ breast cancer cases per 100,000 person-years sounds like a rounding error in any individual decision. But the US alone had about 250,000 unique ART patients in 2022, and globally more than 8 million children have been born from IVF since 1978, implying tens of millions of women treated. The relevant denominator is not one woman; it is millions of them, followed for decades.
At that scale, even small per-person risks matter. Comparable signals in other drug classes — oral contraceptives and clotting risk, hormone replacement and cancer — have prompted label changes and dose adjustments, not because the per-person risk was large but because the population effect was.
For most women, a small possible increase in long-term risk would still be an entirely rational tradeoff for the possibility of having a child. I took on that risk too, by engaging in the process. But the existing follow-up windows are too short to determine the actual risk for the doses women are taking now.
Most importantly, women are owed the option of less exposure. The BMJ data showed early-stage breast cancer rising with the number of cycles. The signal is dose-dependent. Lower-dose stimulation is well established outside the United States, produces comparable outcomes, and reduces the cumulative endocrine load by half to three-quarters. Whatever the long-term answers are, less exposure is a hedge available right now.
Chapter 7: IVF is not automatically safer than conception
What stimulation may do to the pregnancy environment
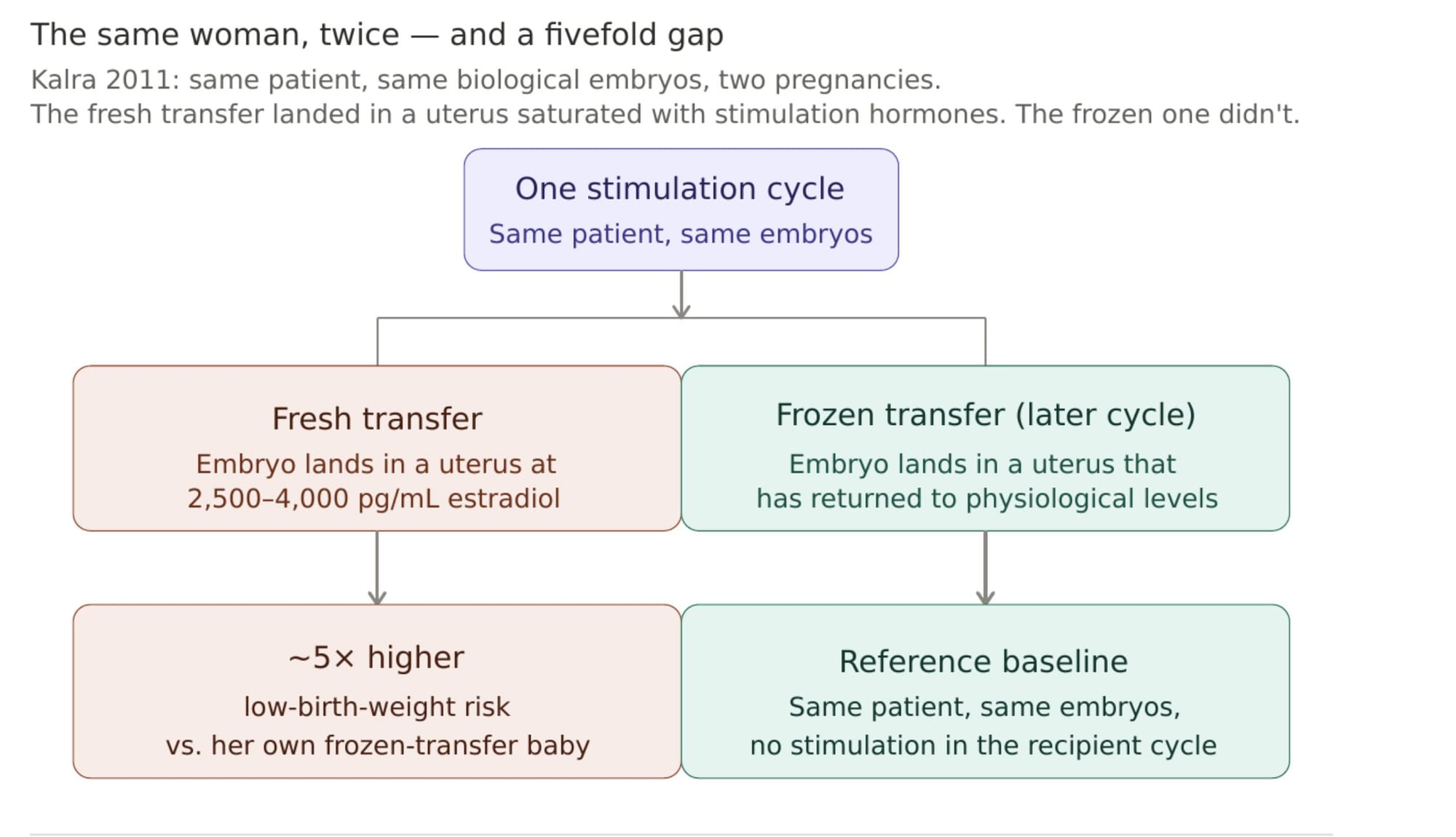
The 2011 SART analysis (Kalra et al.) compared fresh vs. frozen transfers in the same woman, from the same retrieval cycle. Donor-egg recipients, who are not stimulated themselves, showed no such difference.One of the more striking findings in the fertility literature concerns not the woman undergoing stimulation, but the resulting child.Babies born after fresh IVF transfers have consistently been found to have higher rates of low birth weight, preterm delivery, and small-for-gestational-age status than babies born after frozen transfers.
The difficult question has always been why. Is it the stimulation itself, the embryo culture process, the underlying infertility, or something else about the patient population?
A 2011 SART analysis used an unusually elegant design to isolate part of that question. The study identified women who had given birth twice from embryos created in the same retrieval cycle, once after a fresh transfer and once after a frozen transfer. In the fresh-transfer pregnancy, implantation occurred immediately after ovarian stimulation, in a hormonal environment marked by supraphysiologic estrogen levels. In the frozen-transfer pregnancy, implantation occurred later, after the body had returned to a closer-to-baseline physiology.
The difference in outcomes was substantial. The same patient had a markedly higher risk of delivering a low-birth-weight baby after fresh transfer than after frozen transfer. Meanwhile, donor-egg recipients, women receiving embryos created from someone else’s stimulated cycle but who themselves did not undergo ovarian stimulation, showed little difference between fresh and frozen transfer outcomes.
This does not prove with certainty that stimulation itself causes the effect. But it strongly suggests the hormonal environment created by aggressive ovarian stimulation may influence implantation and placental development in ways that matter downstream for the pregnancy.
The mechanism remains debated. What matters clinically is that the signal is sufficiently consistent that many clinics, particularly in Europe, have increasingly moved toward freeze-all strategies: retrieving embryos during the stimulated cycle and then transferring them later in a more baseline hormonal environment. Many American clinics have not, in part because a fresh transfer simplifies scheduling, billing, and the success-rate metric the clinic is measured on. The woman absorbing the difference, again, is the patient.
The “IVF is safer” framing
There is a quieter pull worth naming separately because it increasingly operates on women who are not infertile at all. The result is that some healthy women begin to experience natural conception itself as reckless or biologically inferior — not because the evidence clearly says that, but because the surrounding culture increasingly frames technological mediation as safety.
The logic follows- older eggs carry a higher chromosomal risk, IVF allows embryos to be screened before transfer, therefore IVF must reduce downstream risk compared to natural conception.This is one of the most psychologically powerful versions of the fertility funnel because it frames IVF not as an intervention, but as a prevention..Large population studies do not show that IVF consistently produces healthier babies than natural conception in this age group.
One Australian population-level cohort study of more than 300,000 births found unadjusted birth-defect rates of 7.1% in IVF pregnancies, 9.9% in ICSI pregnancies (where the sperm is manually injected into an egg by the clinic), and 5.7% in spontaneous conceptions. After adjustment for parental infertility and maternal factors, the IVF signal weakened, but the ICSI signal persisted.The broader literature remains mixed, but not in the direction many patients assume.
A 2013 meta-analysis concluded that birth defects remain more common in assisted fertility babies. More recent reviews similarly describe modest but persistent elevations in risks like preterm birth, low birth weight, placental abnormalities, and some congenital anomalies in IVF singletons compared with spontaneous conception, though the extent to which this reflects the procedures themselves versus the underlying infertility remains debated.
The standard objection is that IVF and naturally conceiving populations are fundamentally different- IVF patients are older on average and more medically complex, thus being more likely to have underlying infertility. That objection is correct, and it makes the data difficult to interpret cleanly. But it also means the claim that IVF is broadly safer than natural conception for otherwise healthy older women is much harder to make confidently than fertility marketing suggests.Again, none of this means IVF lacks value. For women with known infertility, recurrent pregnancy loss, or specific genetic indications, these technologies can be transformative. But healthy women begin to experience natural conception itself as reckless or biologically inferior, driven by marketing fear and interventionist culture.
ICSI: the lab procedure most patients don’t realize is optional
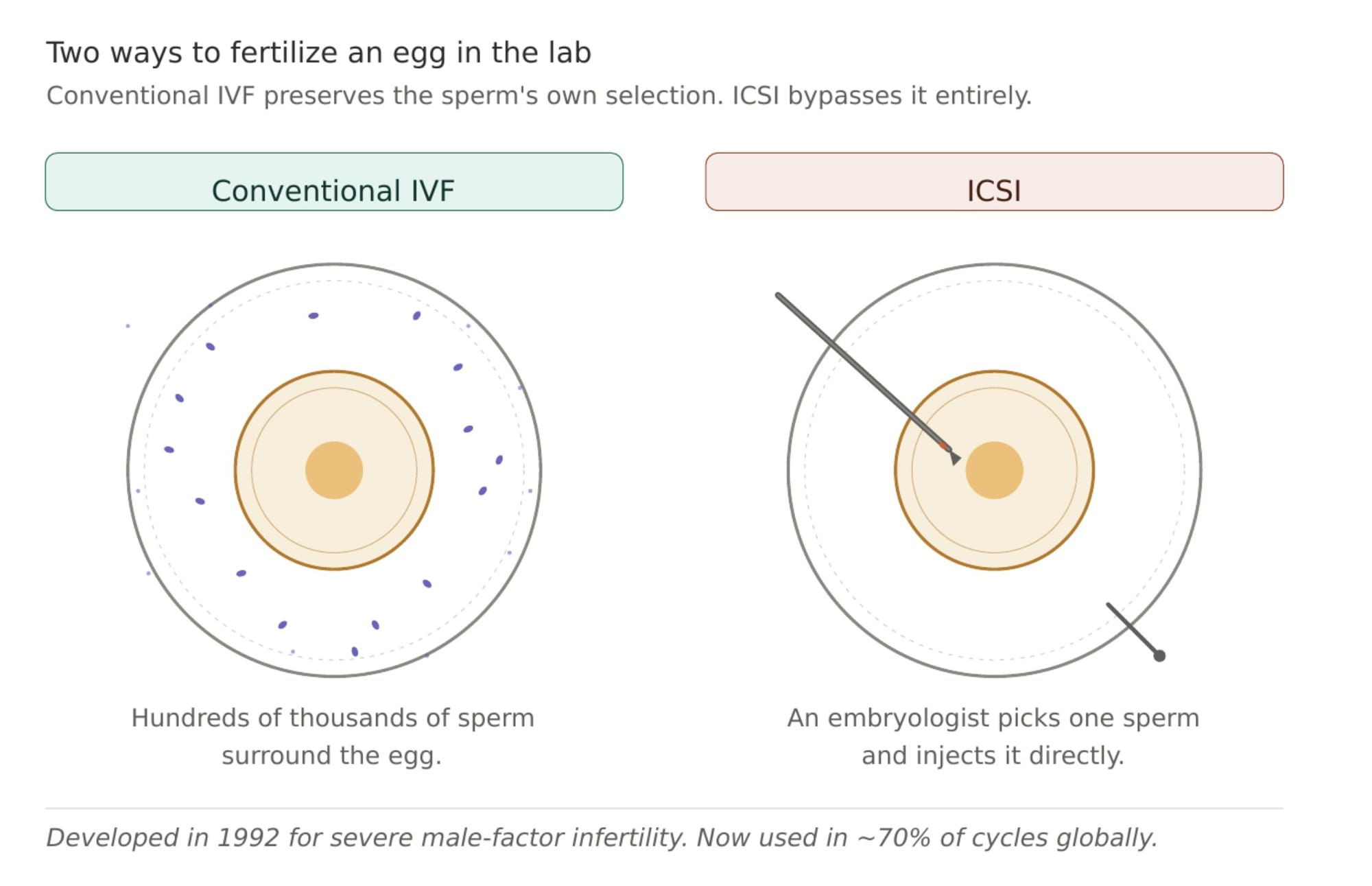
The procedure was developed in the early 1990s for severe male-factor infertility, cases where sperm count or motility was so impaired that fertilization could not reliably occur otherwise. In that setting, ICSI is a genuine breakthrough. The problem is that it gradually expanded far beyond that indication. In the United States, ICSI use rose from 36.4% of IVF cycles in 1996 to 76.2% by 2012, with the largest relative increase occurring in couples without male-factor infertility, where use rose from 15.4% to 66.9% over the same period.
By 2016, CDC data showed ICSI being used in 68–72% of cycles without a male-factor diagnosis, depending on age group.The rationale sounds intuitive: if fertilization is the goal, directly injecting the sperm into the egg seems safer and more controlled.
But the evidence in couples without male-factor infertility is surprisingly weak. A 2021 review by Glenn, Kotlyar, and Seifer at Yale concluded that ICSI should largely be limited to male-factor infertility or prior fertilization failure, citing trial data showing that 33 couples without male-factor infertility would need to undergo unnecessary ICSI to prevent one case of failed fertilization.Randomized trial data points in the same direction.
Three randomized controlled trials in non-male-factor infertility — Bhattacharya 2001, Foong 2006, and Dang 2021 — found no meaningful improvement in pregnancy or live birth outcomes with ICSI over conventional IVF, and a 2023 Cochrane review found no clear live-birth benefit. A 2024 Lancet randomized trial in couples with non-severe male-factor infertility found that ICSI did not improve live birth rates, and ongoing pregnancy was slightly lower with ICSI than with conventional IVF.
Part of the concern is biological. Conventional IVF still preserves a version of natural sperm selection: sperm must reach and penetrate the egg on their own. ICSI bypasses that process entirely. Whether that matters clinically in healthy couples remains debated, but it is notable that a procedure invented for severe pathology became normalized for routine use before strong evidence supporting that expansion existed.
There are also practical incentives pushing clinics toward ICSI. Failed fertilization in a conventional IVF cycle is reputationally damaging for clinics, while ICSI gives laboratories more control over timing and creates a billable add-on that can cost patients an additional $1,500–$2,500 per cycle. A 2024 Reproductive BioMedicine Online review noted that defaulting to ICSI for most patients also simplifies laboratory workflow and reduces the need to maintain expertise in conventional insemination techniques.
I hadn't understood the data well enough to ask questions about ICSI in my own cycle. The clinic initially suggested splitting the eggs 50/50 between conventional IVF and ICSI as a way of comparing fertilization outcomes, which sounded reasonable to me. But while still groggy and recovering from retrieval, the clinic called to say they recommended switching all of the eggs to ICSI, which it may have been. For many patients offered ICSI, that may not be true.
Chapter 8: Why the American system pushes intensity
If gentler stimulation protocols often produce comparable cumulative outcomes with lower hormonal exposure, why do most American women still encounter high-dose IVF as the default?
A central driver of this medication creep is SART data reporting. SART publishes clinic-level success rates that function as de facto marketing metrics in a largely cash-pay US market. Clinics compete for patients on these publicly visible numbers, so they are structurally incentivised to maximise eggs per cycle, which directly requires higher doses and more aggressive stimulation. A clinic using gentler, lower-dose protocols would appear to have “worse” SART numbers even if long-term outcomes and patient safety were comparable or better. SART transparency, intended to protect patients, instead pressures clinics toward ever-higher medication intensity, while patients interpret higher egg counts as better care.
Fertility medicine also sits inside a set of unusually powerful financial incentives that all push in the same direction. Employer-benefits structure pushes intensity further. Fertility benefits have spread rapidly across the tech and professional sectors. The benefits are framed as progressive and family-friendly, and in many ways, they are.
But they also create a use-it-or-lose-it logic around a limited number of funded cycles. If an employer is covering one retrieval worth $20,000 or more, both the clinic and the patient are incentivised to maximise what comes out of that single cycle, which, clinically, translates into pressure for higher doses and larger egg cohorts.
Underneath the employer-benefits layer sits a venture-capital-funded fertility startup ecosystem that has poured billions into consumer-facing fertility companies. The most visible example is Kindbody with a deliberately “spa-like” millennial aesthetic that framed fertility care less like a hospital system and more like a wellness brand. The company expanded rapidly through stylish retail clinics, employer partnerships, and free AMH-testing pop-ups designed to funnel healthy young women into paid fertility services.
But the growth story also exposed the pressures created when fertility clinics operate like venture-backed startups expected to scale quickly and generate recurring revenue. Bloomberg’s 2025 investigation IVF Disrupted: The Kindbody Story described internal pressure around more lucrative procedures, patient complaints about being pushed toward expensive IVF cycles and questionable add-ons. Kindbody is one company, not the whole industry. But the structural incentives it operated under, aggressive growth expectations layered onto a largely cash-pay medical system, extend far beyond a single clinic chain.
None of this means individual doctors are acting in bad faith. Most fertility physicians are operating within the norms of the system in which they were trained. A clinic measured on eggs retrieved per cycle, funded through a largely cash-pay structure, and competing in a consumer market will predictably drift toward protocols that maximise visible output per retrieval.
Chapter 9: What this leaves for an American patient
None of this means IVF or egg freezing are ineffective. It means the version of the protocol commonly presented to a healthy woman in her early-to-mid thirties is often far more aggressive than many patients realise when they first walk into a consultation.High-volume clinics need defaults to function. But it does mean the initial protocol a patient receives is often less individually tailored than many assume.
What surprised me most while writing this essay was how adjustable the system became once someone started asking informed questions. While I was writing this, a friend was about to begin an egg-freezing cycle and had been given her high-dose protocol. She went back to her doctor, asking if a milder protocol would be reasonable. Her doctor discussed it thoughtfully with her and ultimately adjusted the protocol significantly downward.
Should you travel?
Countries like Japan, Spain, the UK, and parts of continental Europe have a longer tradition of mild stimulation, so those approaches are easier to find and more normalised within the system itself.
The cost difference can also be substantial. American fertility care is unusually medication-heavy and largely cash-pay, so conventional IVF cycles in major US cities often cost several times more than lower-intensity cycles abroad, even after accounting for flights and accommodation For some women, especially younger women considering multiple gentler cycles over time, the arithmetic becomes difficult to ignore.
But none of this means women need to leave the United States to pursue a milder approach. Many American fertility doctors are willing to discuss gentler stimulation plans if patients ask informed and specific questions. The problem is less that these approaches do not exist in the US and more that they are not discussed or requested.And there are real tradeoffs to travelling for care. Fertility treatment is physically and emotionally demanding, and doing it in the place where you feel safest, most supported, and most medically comfortable matters too. For some women, that may outweigh any cost advantage or protocol preference abroad.
What does matter enormously, wherever treatment happens, is laboratory quality. In IVF, a significant portion of the outcome depends not just on the stimulation protocol but on how competently the eggs and embryos are handled once they leave the body. Most countries publish some form of clinical outcome data, but reporting systems are inconsistent and often difficult for patients to interpret
.The way I approached it was by downloading clinic outcome data from multiple countries and using AI tools to help normalise and compare the reporting differences so I could evaluate labs against my own priorities rather than against generic marketing claims. Price, branding, and actual laboratory quality are not the same thing. Metrics like fertilization rate, blastocyst conversion, euploidy rate by age, and vitrification survival matter more than the clinic’s social-media presence or headline egg counts. When you don’t know how to interpret clinic data, the nice thing about AI is that it doesn’t get annoyed if you ask the seemingly most basic questions over and over until you get it.
What I ended up doing
The plan I arrived at, after months of reading the literature and speaking with clinics in multiple countries, was this: try to conceive naturally next year, and bank a small number of healthy embryos as a backup against the possibility that age would narrow the number of children I could eventually have. I was never trying to maximise embryo count. I was trying to create enough optionality that I would not feel cornered later by panic or time.
What surprised me was how invisible the alternatives were. Every American clinic I initially spoke with presented conventional high-dose stimulation as essentially the only option. Once I started reading the underlying literature myself, I realised there were materially different philosophies of IVF being practised elsewhere, and, more quietly, by some doctors inside the United States as well.I researched clinics across Japan, Spain, the UK, Belgium, and the Netherlands and did dozens of consultations. Because I was spending time in the US, I decided I would rather do it there if I could find a doctor willing to consider a much gentler protocol. What mattered most to me was not that they automatically agreed with me. It was that they were willing to discuss the evidence seriously, engage with the dose-response data, and adjust the protocol thoughtfully rather than treating maximal stimulation as an unquestionable default.
The protocol itself was relatively simple, and I had three injections total. Not daily, total across the whole process. I took a short course of oral medications, Clomid and letrozole, two widely used oral medications with much longer clinical histories than many newer fertility add-ons. They work indirectly by encouraging the body to produce more of its own FSH and LH rather than flooding the system with large quantities of injectable gonadotropins. Toward the end of the cycle, my doctor recommended adding two low-dose gonadotropin injections to help the leading follicles finish maturing, mixed with a medication to temporarily prevent ovulation so the timing could be controlled, followed by the final trigger shot before retrieval.
Taking shots was never the thing I was trying to avoid. The thing I was trying to avoid was unnecessary medication, drugs layered into the protocol simply because the system defaults toward maximum yield. Three injections at the end of an otherwise gentle cycle did not feel meaningfully comparable to ten or twelve days of high-dose gonadotropins. The cumulative hormonal exposure was a fraction of a conventional cycle.
Physically, the experience was dramatically easier than I had been told to expect IVF could be. I had some mild bloating and little else. No changes in my mood or capabilities. I wrote most of this essay during the process, happily feeling like my normal self. That ease was not about unusually high tolerance or luck. The protocol simply wasn't asking my body to do anything extreme.
I also went into it understanding the tradeoff clearly. Mild stimulation can produce very small egg cohorts, and small cohorts create real laboratory risk- fertilisation failure, arrested development and ending a cycle with no usable embryos at all. I approached the cycle explicitly as an experiment in lower-dose stimulation with no guarantee of yield. I knew I could come out of the process with zero embryos.
What made the tradeoff feel acceptable to me was that the protocol itself was gentle enough that I knew I could simply do it again. Even repeating two or three mild cycles would still leave my cumulative gonadotropin exposure well below a single conventional high-dose cycle. That changed the psychological framework completely. I stopped thinking in terms of extracting the maximum possible number of eggs from one aggressive month and started thinking in terms of working with my body more incrementally over time.
Questions worth asking your fertility doctor
Most reproductive endocrinologists are not careless when they recommend a default protocol. They are operating high-volume practices where standardized starting points are often the only practical way to manage large numbers of cycles safely. Real customization does happen, which is often what monitoring appointments are for. But the starting assumptions still matter.
Decisions made in the first consultation shape the entire trajectory of the cycle. A patient who is informed and asks thoughtful questions can sometimes end up with a meaningfully different protocol from the one they would have received by default.None of the questions below are meant as a “gotchas.” They are simply ways to open a more collaborative conversation and to understand how your doctor thinks about risk, evidence, and intervention intensity.
- Was my AMH retested? AMH can vary meaningfully across time and testing platforms, and a single low reading is a thin basis for irreversible decisions. (Chapter 1)
- Before recommending IVF, did we look at broader contributors to fertility? For example: thyroid function, thyroid antibodies, fasting insulin, vitamin D, ferritin, or other metabolic and inflammatory markers. (Chapter 2)
- Would a milder protocol be reasonable in my case? For example: clomiphene- or letrozole-based stimulation with lower-dose gonadotropins rather than conventional high-dose stimulation. (Chapter 4)
- What is my proposed gonadotropin dose, and what evidence supports that dose for someone with my baselines? ESHRE guidelines caution against routinely escalating beyond 300 IU/day in predicted poor responders. (Chapter 4)
- What trigger strategy are you planning to use, and why? hCG triggers, agonist triggers, and dual triggers have different tradeoffs around OHSS risk and hormonal exposure. (Chapter 4)
- Is ICSI indicated in my case? If so, based on what evidence or male-factor findings? (Chapter 6)
- How flexible is this protocol? If new information emerges during the cycle, or if I have concerns about stimulation intensity, is this a clinic that can adjust? (Chapter 4)
A doctor does not need to agree with every concern in this essay to be a good doctor. But a clinician who is willing to engage seriously with a few informed questions, discuss tradeoffs honestly, and explain their reasoning clearly is usually a very good sign. You can tell a lot by how someone answers a question, especially one that they may not be used to being asked.
Chapter 10: Why the current model may look outdated within a decade
I want to end on something other than a critique. The bigger move underneath this essay is the recognition that ovarian aging is not a fixed feature of human biology that women must work around through ever more aggressive interventions. It is a tractable scientific problem that is now being actively pursued. The ovary ages dramatically faster than the rest of the body, and the medical literature still describes thirty-year-old ovaries with the genuinely jarring term "geriatric".
Researchers have only recently begun to take ovarian aging seriously as a discrete problem, and once you do, the architecture of fertility medicine starts to look provisional. When the Works in Progress essay went viral, I watched the investor reaction online consolidate around “we should be funding more egg freezing clinics.” That is exactly the wrong direction.
Egg freezing clinics are not the future of women’s reproductive health; they are an artefact of the present, a workaround built on top of a constraint that is starting to move.There are several active research streams worth knowing about. Columbia’s VIBRANT trial of low-dose rapamycin, with early data suggesting roughly a 20% reduction in ovarian aging and reports of an extended five-year fertile window. Yale’s ovarian tissue cryopreservation work, where a 2024 modeling paper suggests the procedure could meaningfully delay or, in young enough women, potentially prevent menopause.I
n vitro gametogenesis, generating eggs from skin or blood cells, demonstrated in mice and pursued in humans by both academic labs and companies like Conception and Gameto. And institutional infrastructure- the Buck Institute’s Center for Healthy Aging in Women, is the first dedicated research center in the world targeting ovarian aging as its primary mission. None of these are guaranteed to deliver, and the timelines are uncertain. But if any of these deliver, the framework this essay has been critiquing becomes obsolete.
A woman who could take a generic pill to slow her ovarian aging by five years would make the egg-freezing decision on a completely different timeline. A woman who could bank ovarian tissue at 28 and reimplant it at 45 to push her menopause into her sixties would not need to retrieve and freeze twenty individual eggs in her thirties.
I am, broadly, a tech optimist about all of this. The reason I was not willing to fully rely on future fertility technology in my own decision, even as a woman in my mid-thirties, was not that I doubted the technology would arrive. It was that I worried something might delay its arrival, a regulatory freeze, a war, some shock to the global research apparatus that pushes the timeline out by a decade. I hope and expect science to get there.
Reproductive medicine has historically taken decades to translate biological research into something that helps actual patients. But that's partly a function of the tools the field had when the work began. AI has dramatically sped things up in nearby fields like cancer, drug discovery, and rare disease, and there's good reason to think it'll do the same here. The next decade of fertility medicine will hopefully not look like the previous one
Most women reading this essay still have to make a fertility decision under the existing constraints. I made one and described it honestly. But the conversation I want to be having with my children is one where my peers and I were the last generation who had to navigate American fertility medicine in its current form.The future of women’s health is in extending the working life of the ovary itself. Everything else, eventually, becomes unnecessary.
Appendix: Methodology and AI
I spent the equivalent of a few months full-time on this research, and without AI tools, it would have been impossible to parse so much material on a single topic and bring it all together. To have an AI you could turn loose on medical literature to surface buried results was something I fantasized about ten years ago, while trying to help my father during an acute health crisis. A decade later, something like that exists - but weaklyIf you think AI is really good at research, you have not been asking deep enough questions or stress-testing answers enough. The discipline that made the difference in this essay was learning to stress-test consensus, whether it came from a doctor or from an AI quoting one.
Every time a clinic recommended something, I asked one of the leading AI models whether the evidence supported it. The first answer was almost always a confident yes, here is the research. That confidence was the trap. AI often fabricates citations when asked for sources, stitching together plausible-sounding studies that don't actually exist, without a base document to work from. And the models quietly inherit the biases of the literature they were trained on, which in fertility medicine means a lot of industry-funded research.
Large chunks of general opinion on biomedical science are built on data thinner than people realise: small sample sizes, short follow-up windows, replications that are expensive and rare. Head-to-head comparisons between cheaper and more expensive options are hard to get funded, because the side that would lose has more to lose than the side that would win has to gain. Whole categories of clinically important questions sit unanswered because there isn’t an obvious profit mechanism for the answer.
Scientific understanding does not emerge automatically from scale alone. The bottleneck on AI helping with research is not compute or model capability. Better models trained on broken evidence bases will produce more confident versions of the wrong answers, faster. The constraint everyone is racing to break is not the only constraint that matters. Build the research base, then let the next tools read across it properly.